
")




Description
Also comes with:
- Resources, Contacts, Next Steps with all the Testing Results
- Access to CIRS Group Support with Judy Cho (additional fees apply)
Turnaround Time: 4-6 weeks (lab time is about 3-4 weeks)
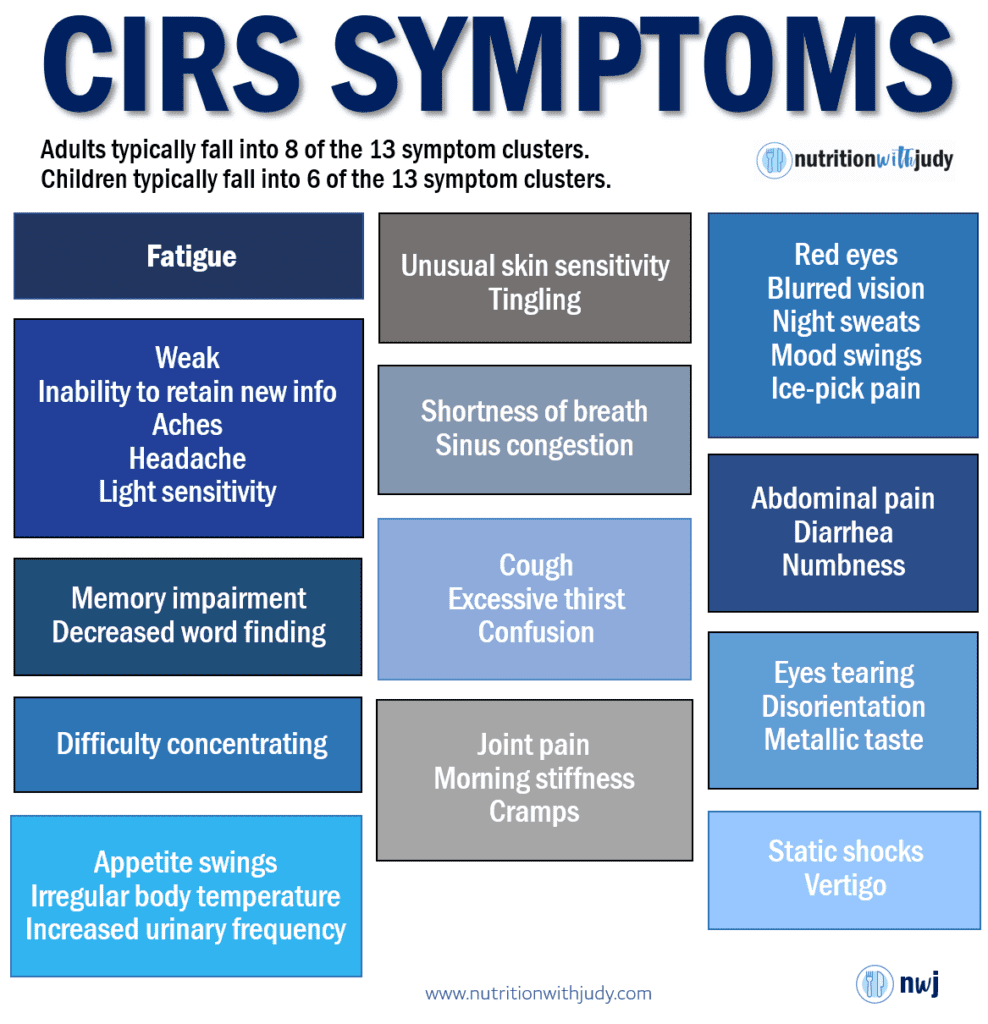
If you are not healing from any particular diet, you may have been exposed to a biotoxin and now suffering from chronic inflammation. Before testing for CIRS through bloodwork, make sure to test for symptoms (see the CIRS Cluster of Symptoms below) and test your vision (VCS Test).
If you have 8 of the 13 symptom clusters and fail the vision test, you are a strong candidate for bloodwork.
The CIRS bloodwork will provide your genetic haplotype to see if you have one (or more) genes that make you more susceptible to chronic inflammation. If you’ve ever been diagnosed with mold, Lyme or MS, you may want to get tested.
NOTE: You only need to test for your haplotype once. For future testing for improvements, you will only need to test a few markers. (e.g., MMP-9, MSH, TGF-Beta 1, etc.)
The following markers will be tested and an overall synthesis of your bloodwork will be provided. Follow-up support will also be provided via email.
HLA DR1/3/4/5, DQ Intermediate Resolution (167120)
- HLA antigens may be correlated with certain disease states or other clinical conditions. It can also be used for screening of transplant candidates and potential donors, transfusion of specifically compatible blood products, and other areas. Researchers have identified hundreds of different versions (alleles) of the HLA-DRB1 gene, each of which is given a particular number such as HLA-DRB1*04:01.
- Note: In his FAQ’s, Dr. Ritchie Shoemaker says, “In assessment of the DRB-1 1-5 over the years (together with its related haplotypes of 10-5 and 103-5, and 1-3 and 1-4) the only variable that reaches statistical significance we have seen is a reduced level of MSH in cases compared to other cases and then to controls.”
- Up to 5% with a Benign haplotype may still get CIRS from mold but will recovery more easily. There are a total of 54 known haplotypes – see page 716 in the book “Surviving Mold”. Alternatively, upon completion of the Biotoxin Test, you’ll be shown the 54 haplotypes.
DHEA-S (Dehydroepiandrosterone Sulfate) (004020)
- Androgen hormones are affected by biotoxins and may be a cause of low energy
Testosterone, Free, Direct with Total Testosterone (140103)
- Androgen hormones are affected by biotoxins and may be a cause of low energy
Human Transforming Growth Factor beta 1 (TGF-b1) (821342)
- Elevated TGF beta-1 indicates an over-active immune response and is a key marker for severity in CIRS. It can change regulatory T cells into pathologic T cells, which then drive further inflammation.
- It also may cause tissue remodeling in multiple tissues in the body. Lowering TGF Beta-1 is critically important due to the potential for long term tissue changes due to the remodeling capacity of this cytokine
Adrenocorticotropic Hormone (ACTH), Plasma (004440)
- An indication of CIRS is dysregulation of primary hormonal systems in the body including the ACTH/cortisol axis, ADH/osmolality control and altered levels of sex hormones like low testosterone
- ACTH is a pituitary hormone that stimulates the production of cortisol from the adrenal glands.
Cortisol (004051)
- Cortisol levels are usually highest between 6 and 8 a.m. and at the lowest around 11 p.m.
- Cortisol is the hormone that is released during stress. It essentially revs up your body so you can handle the stress you are encountering. One of the types of stress you can experience is physiological stress, or negative things that are happening within your metabolism such as low blood sugar or high blood sugar.
Antidiuretic Hormone (ADH), Plasma (010447)
- An indication of CIRS is dysregulation of primary hormonal systems in the body including the ACTH/cortisol axis, ADH/osmolality control and altered levels of sex hormones like low testosterone
- Antidiuretic hormone (ADH) is responsible for regulating the balance of fluid and salt in the body. Other names for ADH include arginine vasopressin (AVP) and vasopressin. Doctors use an ADH test to look for possible underlying causes of fluid and electrolyte imbalances.
Osmolality (002071)
- An indication of CIRS is dysregulation of primary hormonal systems in the body including the ACTH/cortisol axis, ADH/osmolality control and altered levels of sex hormones like low testosterone.
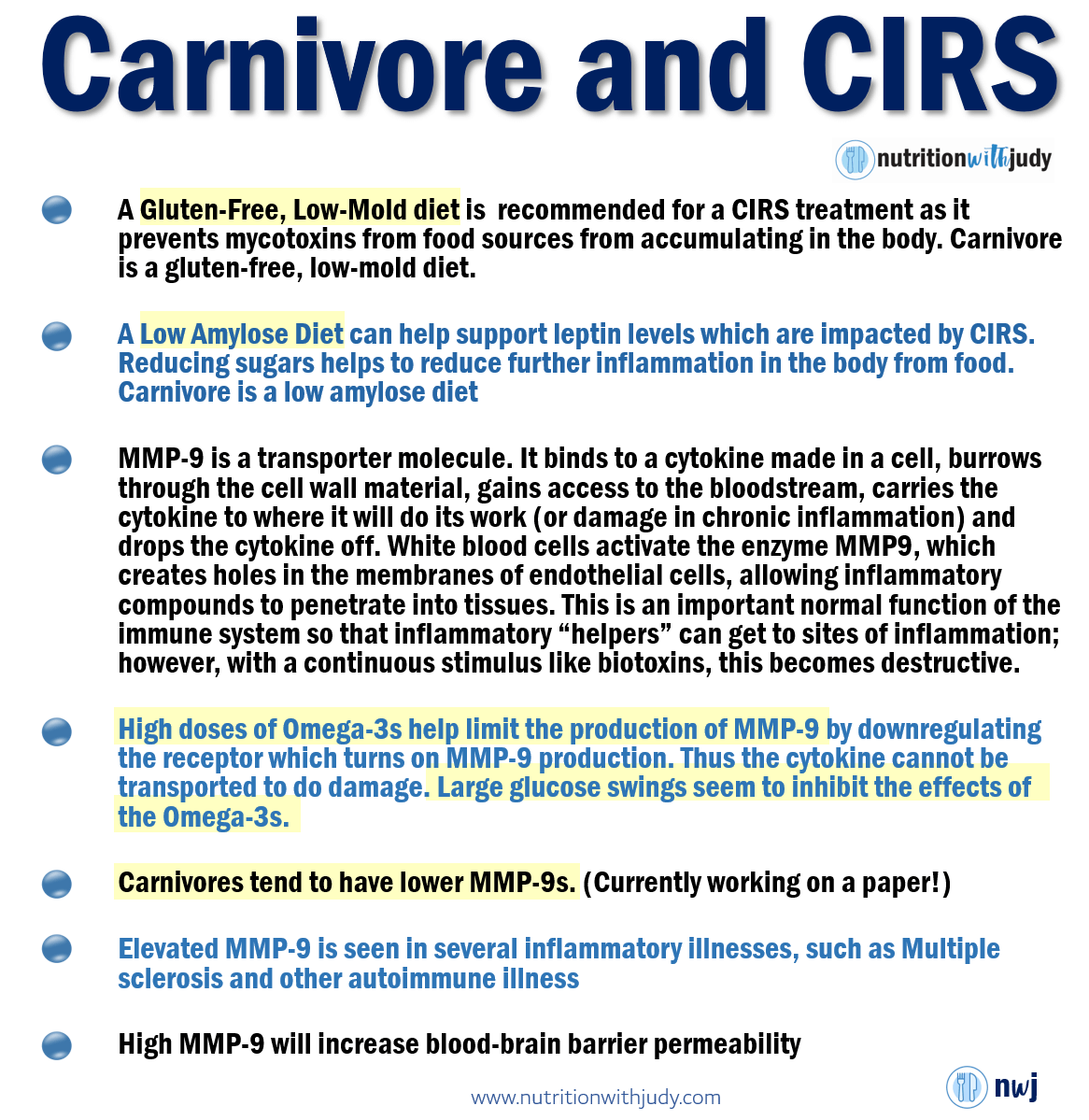
MMP-9 (Matrix Metalloproteinase-9) (500124)
- White blood cells (activated macrophages) activate the enzyme MMP9 which creates holes in the basement membranes of endothelial cells, allowing inflammatory compounds to penetrate into tissues. This is an important normal function of the immune system so that inflammatory “helpers” can get to sites of inflammation; however with a continuous stimulus like biotoxins, this becomes destructive.
Leptin, Serum or Plasma (146712)
- When individuals are struggling with obesity, a decreased amount of leptin may indicate that there is a deficiency contributing to the weight gain. Most people who have a BMI above 30 will usually have increased leptin levels, but about 1 in 10 people are believed to have some level of a deficiency in place instead.
- There may also be a genetic link to the decreased leptin levels found in individuals. This is usually seen when leptin levels are severely low. Testing for leptin typically occurs in the morning because levels are the highest at night. If the leptin blood test is administered in the afternoon, then the test results may show an abnormal level even though their peak circadian rhythm levels are actually in the normal range.
- Leptin Resistance is seen due to disruption of receptors from bombardment with cytokine. This causes dysregulation of MSH and stubborn weight gain.
C-Reactive Protein (CRP), Quantitative (006627)
- CRP measures the C-reactive protein levels in the blood.
- C-reactive protein is a special protein produced by the liver and released into the blood. When there is an inflammation or infection, the C-reactive protein level in the blood plasma increases rapidly. Hence, it is a good biomarker for the identification of acute phase inflammations. Soon after the infection, the level of CRP rises within 2 hours of an adult and persists in the blood plasma for about 18 hours. This rapid increase of CRP level indicates the acute or the first phase of infection. Hence, CRP is known as acute phase protein as well.
Lipase (001404)
- A lipase test, also known as a serum lipase test, can show whether levels of lipase are high. High levels may indicate a problem with the pancreas. The pancreas produces lipase during digestion. This enzyme helps the intestines to break down fats. When the pancreas is inflamed, it secretes extra lipase.
- Higher end is related to pancreas inflammation
- acute pancreatitis
- gallstones gastroenteritis, which occurs when a virus causes inflammation of the stomach
- a problem with the bowel, such as a blockagean ulcer
- cholecystitis, or sudden inflammation of the gallbladder
- celiac disease
- cirrhosis
- pancreatic cancer
- kidney failure
Melanocyte-stimulating Hormone (MSH) (010421)
- Release of this neuroregulatory hormone is controlled by leptin in the pituitary. With biotoxin illness, disruption of the leptin receptor due to an increase in cytokines causes a drop in MSH, a master controller of many functions in the body.
- Low levels of MSH lead to dysregulation of multiple processes causing:
- Problems with sleep patterns and melatonin, leading to disturbed sleep
- Problems with salt and water balance through interaction with ADH/AVP and serum osmolality, leading to increased thirst and urination, palpitations and POTS
- Dysregulation of the immune system with increased inflammatory cytokines, T cell abnormalities, and increase in autoimmunity.
- Increased pain due to decreased endorphin production
- Issues with increased gut permeability
- Reduction in androgens/low testosterone
- Colonization of the nose with MARCoNS
- Weight gain unresponsive to changes in diet and exercise
Complement C4a (004330)
- Activation of the complement system plays an important role in our natural ability to ward off infection and in the pathogenesis of infection and inflammation.1-6 Anaphylatoxins produced as the result of complement activation play a role in a number of infectious and inflammatory conditions including sepsis, ischemia-reperfusion injury, immune complex diseases, and hypersensitivity diseases like asthma.1 Anaphylatoxins are also thought to be important in the pathogenesis of allergy, autoimmunity, neurodegenerative diseases, and cancer.2,3
- Complement activation can occur through three separate mechanisms. The first mechanism to be discovered, referred to as the classical complement cascade, is activated by antigen-antibody complexes.4-6 This was the basis for the name of this system as they serve to “complement” humoral immunity. Alternatively, the complement cascade can be activated directly by contact with bacterial cell surface molecules, including lipopolysaccharide from gram-negative outer membranes, teichoic acid from gram-positive cell walls, zymosan from fungal and yeast cell walls, and some parasite surface molecules. Recently, a third activation mechanism has been characterized in which mannose-binding lectin synthesized by the liver in response to inflammatory macrophage cytokines stimulates the activation of complement.
- Complement cascade activation results in the formation of complement split products C3a, C4a, and C5a.4 These proteins, referred to as anaphylatoxins, facilitate the phagocytosis of immune complexes, viral particles, toxic cell debris, and apoptotic corpses. Anaphylatoxins promote an inflammatory response by binding to complement receptors on granulocytes and macrophages.2 Anaphylatoxins also bind to receptors on mast cells, which trigger the release of histamine, increasing blood vessel permeability and smooth muscle contraction.6 They control the local inflammatory response through the activation of leukocytes and stimulating their chemotaxis to the site of infection.4
- Complement C4a levels can become increased in any condition associated with inflammation.2,3 Normal human pregnancy is associated with evidence of complement activation, with an increase in concentrations of the anaphylatoxins C3a, C4a, and C5a in the maternal circulation.7 Levels of anaphylatoxins C3a and C4a have also been found to be elevated in patients with antiphospholipid syndrome relative to healthy controls.8 Ingram and associates have shown that levels of C4a are increased in patients with multiple sclerosis, especially during relapse.9
- Complement activation split products are present only in trace amounts in normal plasma in vivo.10 It is crucial that samples be collected and stored properly in order to avoid in vitro activation.10 Blood must be drawn directly into tubes containing EDTA at a final concentration of at least 10 mM.10 Citrate and heparin do not block complement activation efficiently and should not be used.10 The addition of nafamostat mesylate (Futhan, FUT-175) further reduces in vitro complement activation.11
In addition, per CIRS provider recommendations, we test these markers to round out your metabolic health testing and provide a comprehensive health report:
- Complete Blood Count (CBC) With Differential (005009)
- Comprehensive Metabolic Panel (CMP-14) (322000)
- Ferritin + Iron + Total Iron-binding Capacity (TIBC) (324741)
- Hemoglobin A1c (HbA1c) (001453)
- Lipid Profile With Non-HDL Cholesterol (343925)
- Magnesium (001537)
- Thyroid Antibodies (Thyroglobulin Antibody + Thyroid Peroxidase (TPO) Antibody) (006684)
- Thyroid Profile With TSH (000620)
Once you purchase the bloodwork, you will receive instructions on the next steps.
While there’s a lot of new information about Chronic Inflammatory Response Syndrome, if you work with the NwJ team, you will be provided with CIRS resources and support.
Reviews
There are no reviews yet.