
Description
This is a retest and should not be used for initial CIRS diagnosis. If you want the full test, you can take find the comprehensive CIRS panel, here.
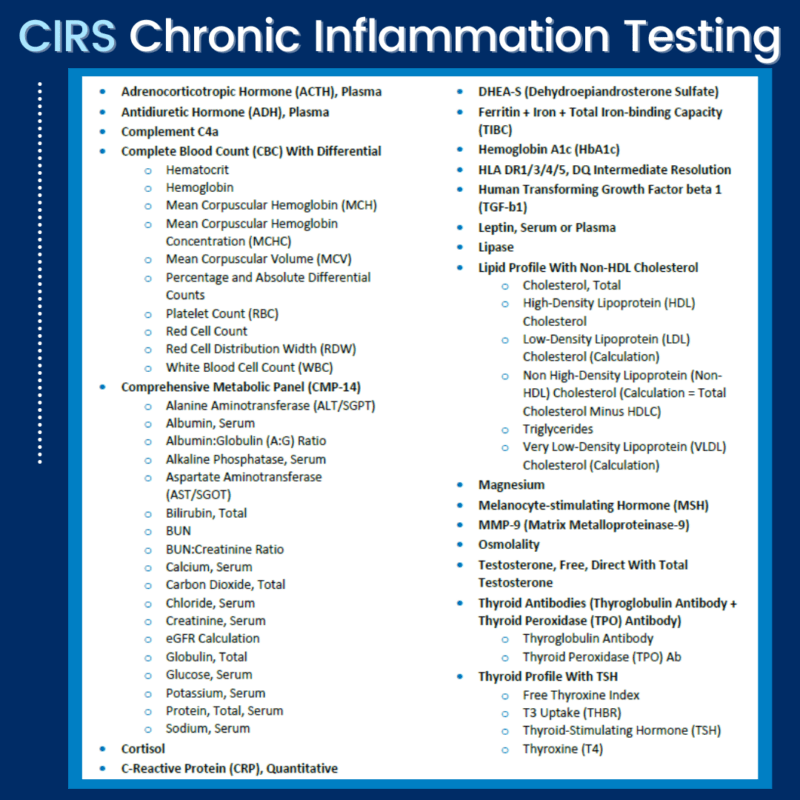
This panel provides a partial snapshot of the CIRS bloodwork to determine status updates on inflammatory markers for CIRS.
All tests from Nutrition with Judy include a detailed analysis (notes) that include Nutrition with Judy explanations, dietary and supplement recommendations, as well as customized next steps based on your test results.
The following markers will be tested and an overall synthesis of your bloodwork will be provided. Follow-up support will also be provided via email.
Human Transforming Growth Factor beta 1 (TGF-b1) (821342)
- Elevated TGF beta-1 indicates an over-active immune response and is a key marker for severity in CIRS. It can change regulatory T cells into pathologic T cells, which then drive further inflammation.
- It also may cause tissue remodeling in multiple tissues in the body. Lowering TGF Beta-1 is critically important due to the potential for long term tissue changes due to the remodeling capacity of this cytokine
MMP-9 (Matrix Metalloproteinase-9) (500124)
- White blood cells (activated macrophages) activate the enzyme MMP9 which creates holes in the basement membranes of endothelial cells, allowing inflammatory compounds to penetrate into tissues. This is an important normal function of the immune system so that inflammatory “helpers” can get to sites of inflammation; however with a continuous stimulus like biotoxins, this becomes destructive.
Melanocyte-stimulating Hormone (MSH) (010421)
- Release of this neuroregulatory hormone is controlled by leptin in the pituitary. With biotoxin illness, disruption of the leptin receptor due to an increase in cytokines causes a drop in MSH, a master controller of many functions in the body.
- Low levels of MSH lead to dysregulation of multiple processes causing:
- Problems with sleep patterns and melatonin, leading to disturbed sleep
- Problems with salt and water balance through interaction with ADH/AVP and serum osmolality, leading to increased thirst and urination, palpitations and POTS
- Dysregulation of the immune system with increased inflammatory cytokines, T cell abnormalities, and increase in autoimmunity.
- Increased pain due to decreased endorphin production
- Issues with increased gut permeability
- Reduction in androgens/low testosterone
- Colonization of the nose with MARCoNS
- Weight gain unresponsive to changes in diet and exercise
Complement C4a (004330)
- Activation of the complement system plays an important role in our natural ability to ward off infection and in the pathogenesis of infection and inflammation.1-6 Anaphylatoxins produced as the result of complement activation play a role in a number of infectious and inflammatory conditions including sepsis, ischemia-reperfusion injury, immune complex diseases, and hypersensitivity diseases like asthma.1 Anaphylatoxins are also thought to be important in the pathogenesis of allergy, autoimmunity, neurodegenerative diseases, and cancer.2,3
- Complement activation can occur through three separate mechanisms. The first mechanism to be discovered, referred to as the classical complement cascade, is activated by antigen-antibody complexes.4-6 This was the basis for the name of this system as they serve to “complement” humoral immunity. Alternatively, the complement cascade can be activated directly by contact with bacterial cell surface molecules, including lipopolysaccharide from gram-negative outer membranes, teichoic acid from gram-positive cell walls, zymosan from fungal and yeast cell walls, and some parasite surface molecules. Recently, a third activation mechanism has been characterized in which mannose-binding lectin synthesized by the liver in response to inflammatory macrophage cytokines stimulates the activation of complement.
- Complement cascade activation results in the formation of complement split products C3a, C4a, and C5a.4 These proteins, referred to as anaphylatoxins, facilitate the phagocytosis of immune complexes, viral particles, toxic cell debris and apoptotic corpses. Anaphylatoxins promote an inflammatory response by binding to complement receptors on granulocytes and macrophages.2 Anaphylatoxins also bind to receptors on mast cells, which trigger the release of histamine, increasing blood vessel permeability and smooth muscle contraction.6 They control the local inflammatory response through activation of leukocytes and stimulating their chemotaxis to the site of infection.4
- Complement C4a levels can become increased in any condition associated with inflammation.2,3 Normal human pregnancy is associated with evidence of complement activation, with an increase in concentrations of the anaphylatoxins C3a, C4a, and C5a in the maternal circulation.7 Levels of anaphylatoxins C3a and C4a have also been found to be elevated in patients with antiphospholipid syndrome relative to healthy controls.8 Ingram and associates have shown that levels of C4a are increased in patients with multiple sclerosis, especially during relapse.9
- Complement activation split products are present only in trace amounts in normal plasma in vivo.10 It is crucial that samples be collected and stored properly in order to avoid in vitro activation.10 Blood must be drawn directly into tubes containing EDTA at a final concentration of at least 10 mM.10 Citrate and heparin do not block complement activation efficiently and should not be used.10 The addition of nafamostat mesilate (Futhan, FUT-175) further reduces in vitro complement activation.11
DHEA-S (Dehydroepiandrosterone Sulfate) (004020)
- Androgen hormones are affected by biotoxins
Once you purchase the bloodwork, you will receive instructions on how to get testing done.
While there’s a lot of new information about Chronic Inflammatory Response Syndrome, if you do some of the testing with Nutrition with Judy, you will be provided with all her CIRS resources and support.
Reviews
There are no reviews yet.